HIV nocturnal pain/ drop attacks/
nocturnal pain/ drop attacks/ speaking/ swallowing problem
speaking/ swallowing problem
dizziness cancer/ inflammatory arthritis
cancer/ inflammatory arthritis
TB
weight loss/ fevers
less than 20/ more than 55
double vision
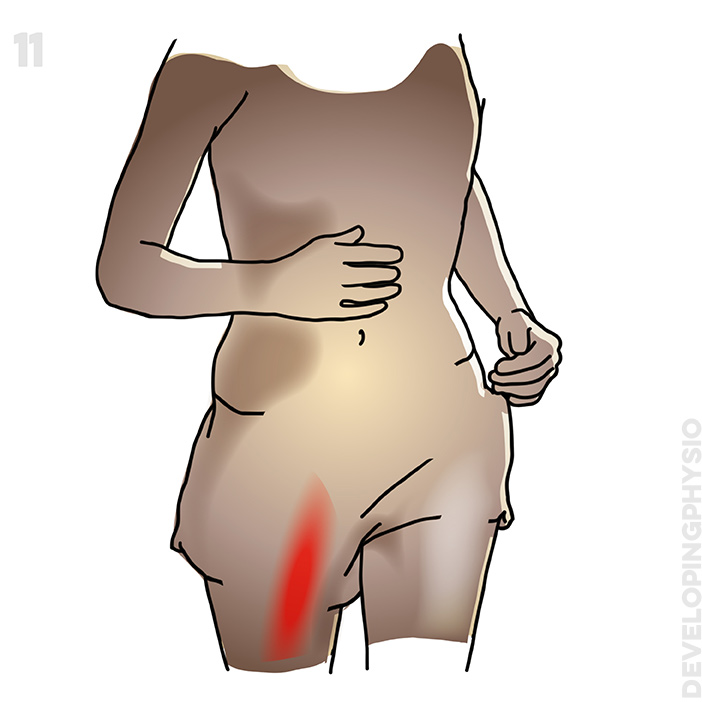
severe pain
spinal cord compression
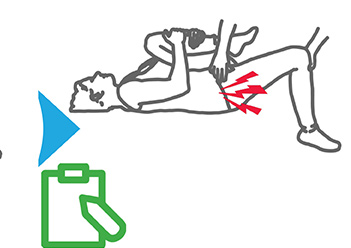
significant vertebral tenderness
neck trauma/ surgery
preceding trauma or neck surgery
bladder/bowel incontinence
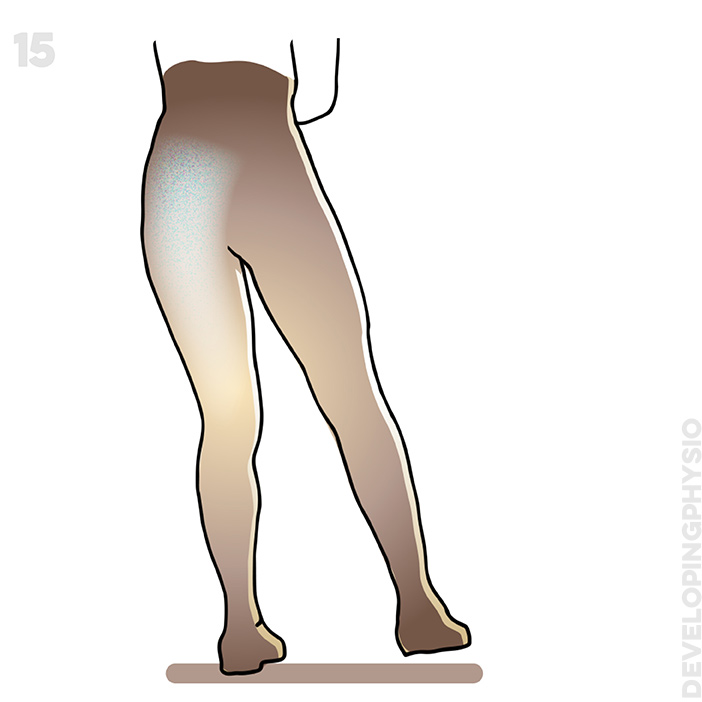
loss of feeling in both legs
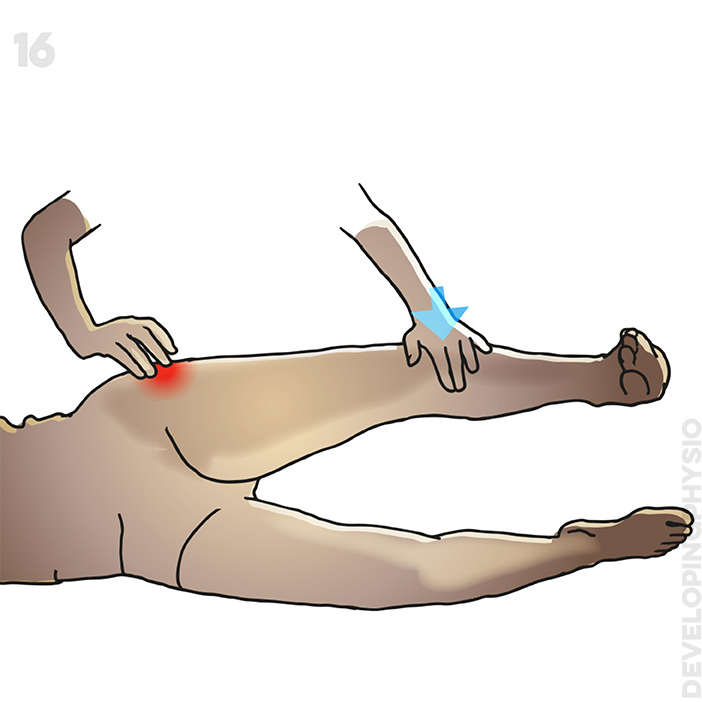
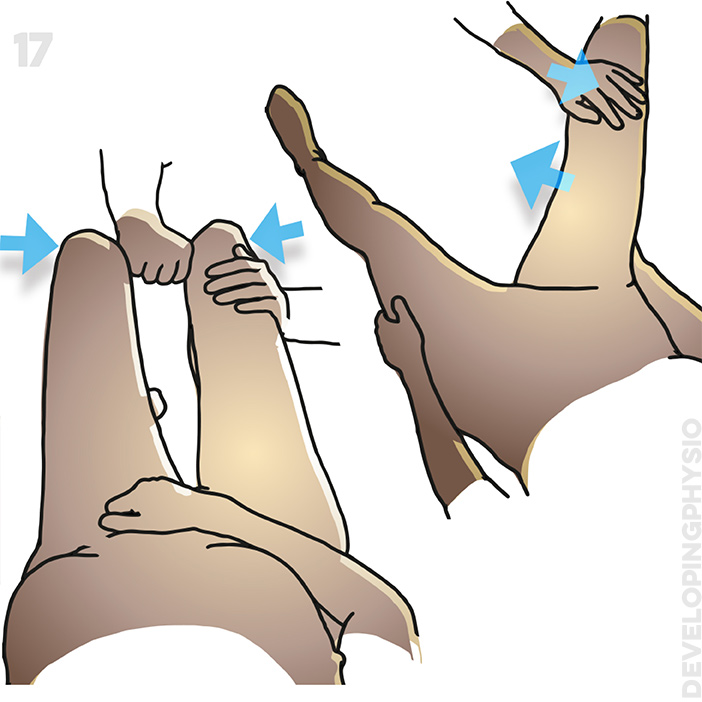
 bjective assessment
bjective assessment

Please seek medical help if any of the above apply or else confirm that you have checked that none do.